

Background
Job-appropriate education and training is essential for all positions involved in clinical research. Education refers to formal degree programs offered by universities and similar institutions; training is defined as skill-building or professional development sessions or courses that are provided outside of formal degree programs. Clinical research competencies consist of skills that are based on practice and experience in the respective professions, as well as a fundamental knowledge of the International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH) Guideline for Good Clinical Practice (GCP) (ICH-GCP) and the regulatory requirements of each country as a reference. Recently, the Joint Task Force for Clinical Trial Core Competency (JTF competency) has issued the core competencies of various clinical research professionals as eight domains and 47 subdomains. Within each domain are specific competency statements that are expressed as a “Basic”, “Skilled” and “Advanced” level along with specific job skills.1,2
The Society for Clinical Data Management (SCDM),3 an international society for data managers, previously reported on the competencies and basic knowledge required of clinical data management (CDM) personnel at annual meetings (SCDM competency).4 Zozus et al.5 conducted a detailed competency survey based on the SCDM competencies, which targeted participants of the SCDM Annual Conference, and have reported the results. The SCDM has also issued a White Paper on the future as well as the current situation.6,7 eSource, artificial intelligence (AI), and other skills newly required for CDM are not currently covered by the Good Clinical Data Management Practice (GCDMP©).8 CDM is also required to keep up with these new technologies. Valenta et al.9 propose competencies related to managing electronic health records and big data, which have seen remarkable advancements in biomedical informatics within the activities of the Clinical and Translational Science Award (CTSA) program in the United States.
In Japan, pharmaceutical companies, and contracted research organizations (CROs) have their own education and training programs for CDMs, but there have been few reports on the generalization of the programs. In addition, some graduate schools of the Academic Research Organizations (AROs) in Japan have provided educational programs for CDM personnel, but as a result of the shortage of human resources it is difficult to provide stable and continuous on-the-job training (OJT) for CDMs in AROs. In Japan, the operational funding for each ARO is covered by resources from affiliated medical institutions and time-limited public funds based on clinical development projects. Consequently, the funds available for hiring personnel are not always stable, and in the case of fixed-term employment, resulting in a high turnover rate and difficulty in continuing to pursue a career. To obtain the necessary competencies for data managers in AROs in Japan, it is important to clarify the competencies and to specify the necessary education programs. So far, the Japan Agency for Medical Research and Development (AMED) has developed a curriculum for data managers10 based on Good Clinical Data Management Practice (GCDMP©), published by SCDM, but its learning objectives were not developed with sufficient awareness of competencies.
AMED has developed a business plan for the development of indicators to evaluate the functions of ARO. ARO’s data managers in Japan have been surveyed for competencies to be part of their function. However, Zozus et al.5 surveyed participants at the SCDM conference, and since only 4–5% of the participants were from Japan, it is not possible to apply the survey as it is to the current competencies of data managers in Japan. We therefore decided to investigate JTF competency and SCDM competency among data managers in the country to clarify the Japanese regional context in these competencies and the required competencies.
Methods
Study design
The study was designed as a survey of project for evaluation of the personnel and infrastructure related to clinical development in academic medical institutions and other companies and organizations within Japan. The survey was administered as an anonymousweb-based questionnaire using the REDCap system (Vanderbilt University, USA). As such, the study was declared as “not involving human subjects” by the Osaka and Tohoku University Review Board (protocol Number 19255), and informed consent of respondents through questionnaire responses was provided with sufficient explanation.
Questionnaire Development
JTF competency and SCDM competency surveillance questionnaires were translated into Japanese by clinical research expert members that consisted of CDM personnel, clinical research associates (CRAs), biostatisticians and investigators in Japan. Each questionnaire item consisted of four sections, demographic (10 items), types of data managed today and in the future (19 items), seven tasks in CDM (67 sub-tasks) (Table 1) and foundational knowledge for CDM (26 items), from the 2018 CDM Task Analysis Questionnaire items by Zozus et al.5 and JTF core competencies (47 subdomains). The demographic section consisted of the following questionnaire: type of affiliation (current and previous), years of experience as a CDM personnel (lead CDM personnel or not), number of projects engaged as a CDM personnel (lead CDM personnel or not). JTF competency and SCDM competency, for the respondents, in the section on demographic, we decided to compare the “early to mid” and “mid to late” carriers by carrier level for each item as a self-rated method of selection. The second section asked questions to indicate the types of data the respondents managed at the time of the survey and the types of data they envisioned managing in the future. The responses included clinical data from case report forms (CRFs), patient reported data (PRO/ePRO), data from medical devices, electronic health record (EHR) data, and social media data. In the third section, for each of the 67 SCDM subtasks, the respondent was asked if they were engaged or not at the time of the survey. In the fourth section, for each of the 47 JTF subdomains, questions were asked at the three levels identified by the JTF (fundamental, skilled and advanced) and “not applicable”. The fifth section of the survey regarded foundational knowledge topics that were needed to implement CDM, such as clinical research fundamentals, data quality fundamentals and regulatory requirements.
Task Category and Details of SCDM.
| Task Category | # | Sub-tasks | # | Sub-tasks |
|---|---|---|---|---|
| 1. Design | 1–1 | Identify data to be collected | 1–2 | Define study data elements |
| 1–3 | Design data collection forms | 1–4 | Drafts CRF completion guide | |
| 1–5 | Annotate forms | 1–6 | Design workflows & data flows | |
| 1–7 | Write/mtn. study procedures | 1–8 | Write/maintn. Data Mgt Plan | |
| 1–9 | Specify logical data storage structures | 1–10 | Specify data entry screens | |
| 1–11 | Specify edit checks | 1–12 | Specify reports | |
| 1–13 | Write data transfer specification | 1–14 | Specify other programming | |
| 1–15 | Write or maintain org. SOPs | 1–16 | Select data standards | |
| 1–17 | Implement data standards | 1–18 | Develop data standards | |
| 1–19 | Manage org. data standards | 1–20 | Responds to audit findings | |
| 1–21 | Defines in-process data QC | |||
| 2. Progarmming | 2–1 | Program database tables | 2–2 | Program data entry screens |
| 2–3 | Program edit checks | 2–4 | Program reports | |
| 2–5 | Program ad hoc SQL queries | 2–6 | Program data imports | |
| 2–7 | Program data transformation | 2–8 | Program data extracts | |
| 3. Process | 3–1 | Collect study data | 3–2 | Enter data |
| 3–3 | Import and export data | 3–4 | Integrate or link data | |
| 3–5 | Reconcile data e.g., lab, safety | 3–6 | Impute data | |
| 3–7 | Transform data | 3–8 | Code data, e.g., medications adverse events, other data | |
| 3–9 | Identify data discrepancies | 3–10 | Query sites re discrepancies | |
| 3–11 | Update database | 3–12 | Measure and report data quality | |
| 3–13 | Applies analytics to identify data & operational problems | 3–14 | Manage data system access and privileges | |
| 3–15 | Curate and archive or share study data | |||
| 4. Testing | 4–1 | Draft test plans and test data | 4–2 | Execute and document tests |
| 5. Training | 5–1 | Facilitates understanding of data management processes | 5–2 | Designs, develops, delivers and evaluates training |
| 6. Project Management | 6–1 | Define & manage scope of work | 6–2 | Select and manage vendors |
| 6–3 | Projects workload | 6–4 | Establishes and manages timelines | |
| 6–5 | Coord. System/DM start-up | 6–6 | Coord. Data collection and processing | |
| 6–7 | Coordinate Site data close-out | 6–8 | Coordinate Database lock | |
| 6–9 | Coordinate Data archival or sharing | 6–10 | Implement new data system | |
| 6–11 | Track and report study data status and metrics | 6–12 | Identifies & manages data risk | |
| 6–13 | Prepares for and hosts audits | 6–14 | Plans and runs meetings | |
| 6–15 | Prepare deliver presentations | 6–16 | Drafts, maintains, and supports project communication plan | |
| 7. Review | 7–1 | Review study documents such as protocols and consent forms to identify impact on data | 7–2 | Review data and data descriptions in Tables, Listings Figures and Clinical Study Reports for accuracy |
| 7–3 | Review CDM work and provide feedback |
Survey Distribution
Notification of the questionnaire survey to CDM personnel in Japan was distributed using the mailing lists of the SCDM Japan branch, the ARO network in Japan, and the Japan Pharmaceutical Manufacturers Association. The survey period was from November 20 to December 3, 2019.
Statistical Analysis
The differences in competencies between early-to-mid and mid-to-late career CDM personnel are expected, the statistical analysis allows us to formally document these variations, particularly across different organizational types such as AROs, CROs, and pharmaceutical companies. These differences are critical as they influence the design and implementation of competency-based training programs tailored to the specific needs of each career stage and organization type. All analyses were prespecified in the study protocol. All respondents’ demographics and characteristics were summarized. Categorical variables were described as counts and proportions and were compared by chi-square test. The significance level was set at 0.05 (two-sided). Statistical analysis was performed using JMP Pro (SAS) Ver. 12.2 (SAS Institute, USA). The study is exploratory in nature, and thus, a consideration of the multiplicity of tests was not performed.
Results
Characteristics of respondents
In total, 124 CDM personnel responded to the survey. The affiliations of the CDM personnel who responded to the questionnaire items were well balanced among AROs (50 (40%)), CRO (36 (29%)) and pharmaceutical companies (38 (31%)). Of the 124 respondents, 118 (95%) were engaged in CDM work at the time of the questionnaire survey. 70 CDM personnel self-categorized as being in their mid-to-late career; 54 were in their early to mid career. CDM career level by self-assessment was linked to whether one had less or more than 5 years of CDM experience (Table 2). The overall trend was for the majority of respondents from AROs to rate themselves as “early to Mid” career and for respondents from pharmaceutical companies to rate themselves as being in their “Mid to Late” careers.
Characteristics of respondents.
| Types of affiliations of CDM personnel | AROs | CROs | Pharmaceuticals |
|---|---|---|---|
| N (%) | 50 (40) | 36 (29) | 38 (31) |
| Experienced years of CDM by each affiliation | |||
| 0–4 years | 29 (58) | 10 (28) | 8 (21) |
| 5–9 years | 11 (22) | 11 (30) | 4 (11) |
| ≧10 years | 10 (20) | 15 (42) | 26 (68) |
| Current/Previous | 50/0 | 34/2 (94/6) | 34/4 (89/11) |
| Early to Mid/Mid to Late | 32/18 (64/36) | 14/22 (39/61) | 8/30 (21/79) |
Differences in SCDM tasks between early-to-mid- and mid-to-late career CDM personnel
Among the 67 sub-tasks, 38 (57%) showed a statistically significant difference between the early-to-mid career and mid-to-late career group (Figure 1 and Table 1). This difference was particularly pronounced in the design tasks related to data flow and procedure development, training, project management, and review tasks. In the design task, most of the mid-to-late career CDM personnel reported that the core tasks for individual research included identifying data to be collected (52 (74.3%) vs. 22 (39.3%), p < 0.0001) and defining study data elements (45 (64.3)% vs. 16 (28.6%), p < 0.0001), as well as determining organizational Standard Operating Procedures (SOPs) (47 (67.1%) vs. 14 (25.9%), p < 0.0001) and managing organizational data standards (46 (65.7%) vs. 9 (16.1%), p < 0.0001). In the training task, mid-to-late career CDM personnel were involved in the facilitation of other CDM personnel on data management procedures (53 (75.7%) vs. 27 (48.2%), p = 0.0014); in the project management section, mid-to-late career respondents were involved in the overall data management of implementation in individual researches, such as defining and managing scope of work (54 (77.1%) vs. 16 (28.6%), p < 0.0001), selecting and managing vendors (43 (61.4%) vs. 16 (28.6%), p < 0.0001), establishing and managing timelines (58 (82.9%) vs. 25(44.6%), p < 0.0001), and project work load (32 (45.7%) vs 4 (7.1%), p < 0.0001). There was no significant difference of competency between the two groups for SCDM tasks that related to procedures such as programming, validation, and data collection processes.
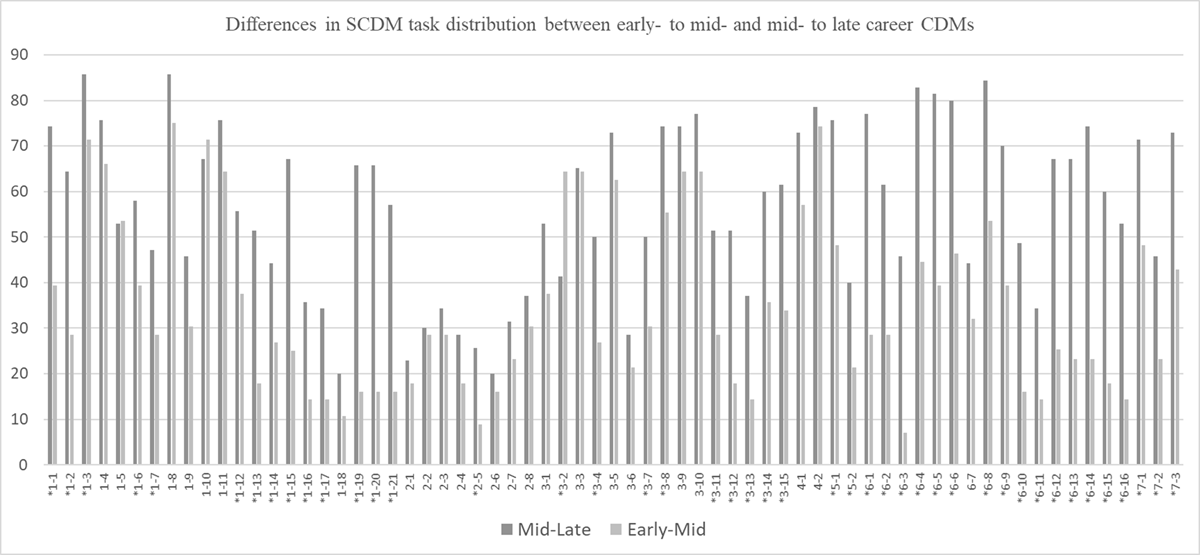
Differences in SCDM task distribution between early- to mid- and mid- to late career CDMs.
(* means that there is a statistically significant difference between the two groups.)
Differences in JTF competencies between early-to-mid and mid-to-late career CDM
Twenty-seven (57%) of both respondent groups (early-to-mid and mid-to-late career CDMs) engaged in the subdomains of the JTF competency, especially in domain 1 “Scientific Concepts and Research Design” and domain 6 “Data management and Informatics” in competencies related to scientific perspectives and policy decisions regarding quality control (Table 3). No significant statistical differences were found between the two groups in the majority of domain 2 “ethical and participant safety considerations”, domain 3 “investigational products development and regulation” or domain 5 “study and site management (Supplemental Table 2).
Differences in JTF core competencies in domain 1 and 6 between “Early- to Mid” (N = 54)- and “Mid- to Late” (N = 70) career of CDM personnel.
| Domains and detailed JTF core competencies | Competency level of statements | Early to Mid N = 54 (%) |
Mid to Late N = 70 (%) |
p-value | |
|---|---|---|---|---|---|
| Domain 1: Scientific Concepts and Research Design | 1.1 Apply principles of biomedical science to investigational product discovery and development and health-related behavioral interventions | Not Applicable | 22 (41) | 5 (7) | <0.0001 |
| Fundamental | 18 (33) | 23 (33) | |||
| Skilled | 11 (20) | 34 (49) | |||
| Advanced | 3 (6) | 8 (11) | |||
| 1.2 Identify scientific questions that are potentially testable clinical research hypotheses | Not Applicable | 8 (15) | 8 (12) | <0.0001 | |
| Fundamental | 29 (54) | 12 (17) | |||
| Skilled | 15 (28) | 28 (40) | |||
| Advanced | 2 (4) | 22 (31) | |||
| 1.3 Identify the elements and explain the principles and processes of designing a clinical study | Not Applicable | 6 (12) | 5 (7) | <0.0001 | |
| Fundamental | 24 (44) | 7 (10) | |||
| Skilled | 19 (35) | 24 (34) | |||
| Advanced | 5 (9) | 34 (49) | |||
| 1.4 Critically analyze clinical study results | Not Applicable | 26 (49) | 28 (40) | 0.0474 | |
| Fundamental | 19 (35) | 15 (21) | |||
| Skilled | 5 (9) | 16 (23) | |||
| Advanced | 4 (7) | 11 (16) | |||
| Domain 6: Data Management and Informatics | 6.1 Describe the role and importance of statistics and informatics in clinical studies | Not Applicable | 13 (24) | 2 (3) | <0.0001 |
| Fundamental | 28 (52) | 10 (14) | |||
| Skilled | 1 (2) | 2 (3) | |||
| Advanced | 12 (22) | 56 (80) | |||
| 6.2 Describe the origin, flow, and management of data through a clinical study | Not Applicable | 8 (15) | 3 (4) | <0.0001 | |
| Fundamental | 34 (63) | 20 (29) | |||
| Skilled | 6 (11) | 15 (21) | |||
| Advanced | 6 (11) | 32 (46) | |||
| 6.3 Describe best practices and resources required for standardizing data collection, capture, management, analysis, and reporting throughout all stages of a clinical study | Not Applicable | 15 (28) | 7 (10) | 0.0070 | |
| Fundamental | 16 (30) | 13 (19) | |||
| Skilled | 5 (9) | 7 (10) | |||
| Advanced | 18 (33) | 43 (61) | |||
| 6.4 Describe, develop, and implement processes for data quality assurance | Not Applicable | 17 (31) | 13 (19) | <0.0001 | |
| Fundamental | 15 (28) | 2 (3) | |||
| Skilled | 14 (26) | 16 (23) | |||
| Advanced | 8 (15) | 39 (55) | |||
Differences in SCDM task distribution among affiliation type of CDM personnel
The distribution of SCDM tasks by CDM personnel’s affiliation type showed significant differences in work tasks among the AROs, CROs, and pharmaceuticals in the design, data processing, and project management areas of the survey. More CDM personnel were engaged in project management tasks in pharmaceutical companies than in AROs and CROs (Supplemental Table 3).
Types of data to be managed
The second section of the survey probed the types of data managed by respondents. All respondents indicated one or more types of data that they manage today. However, most of them do not have experiences of utilizing CDM infrastructures for real world data (RWD) (Figure 2). It was found that the types of data managed currently by CDM personnel which include new technologies such as ePRO, clinical laboratory data (including pharmacokinetic and biospecimen tracking), data from central reading centers, data from personal wearable devices, data from other central “Core” labs, and reference data (such as controlled terminologies) vary significantly depending on the career stage of the respondent (Supplemental Table 4). Although the use of data from medical institutions (eg, CRFs, imaging data and laboratory data) was commonly confirmed across all affiliations, the use of ePRO data was observed relatively more frequently in pharmaceutical companies and CROs than in AROs (pharmaceuticals/CRO/ARO, 21(54%) /20(56%)/ 21(45%)).
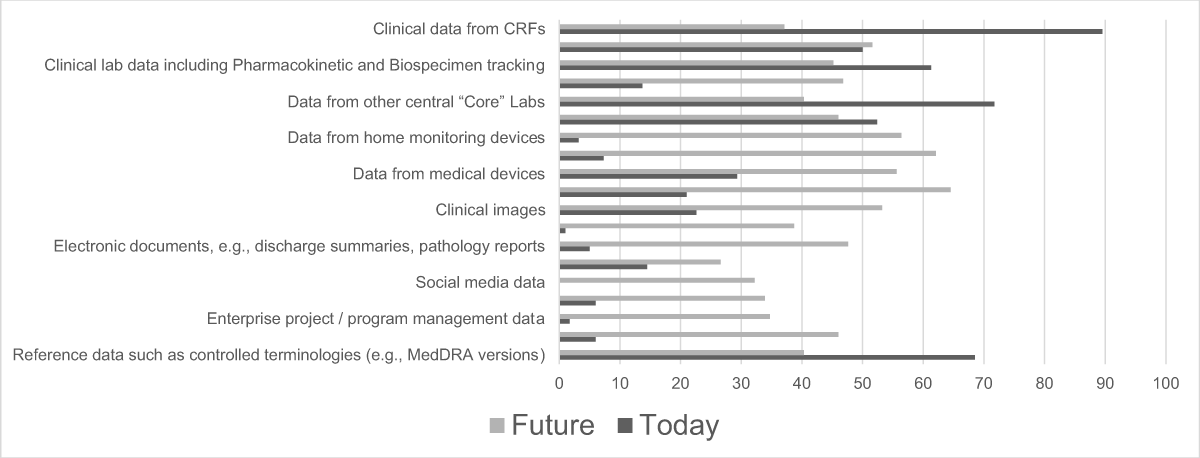
Types of data managed by respondents.
Foundational knowledge
It was found that CDM personnel in Japan were strongly interested in regulation (48.4%), data quality (46.8%), basic research knowledge (46%), and drug development in disease areas (45.2%), but not in new technologies related to software and computer systems. (Figure 3).
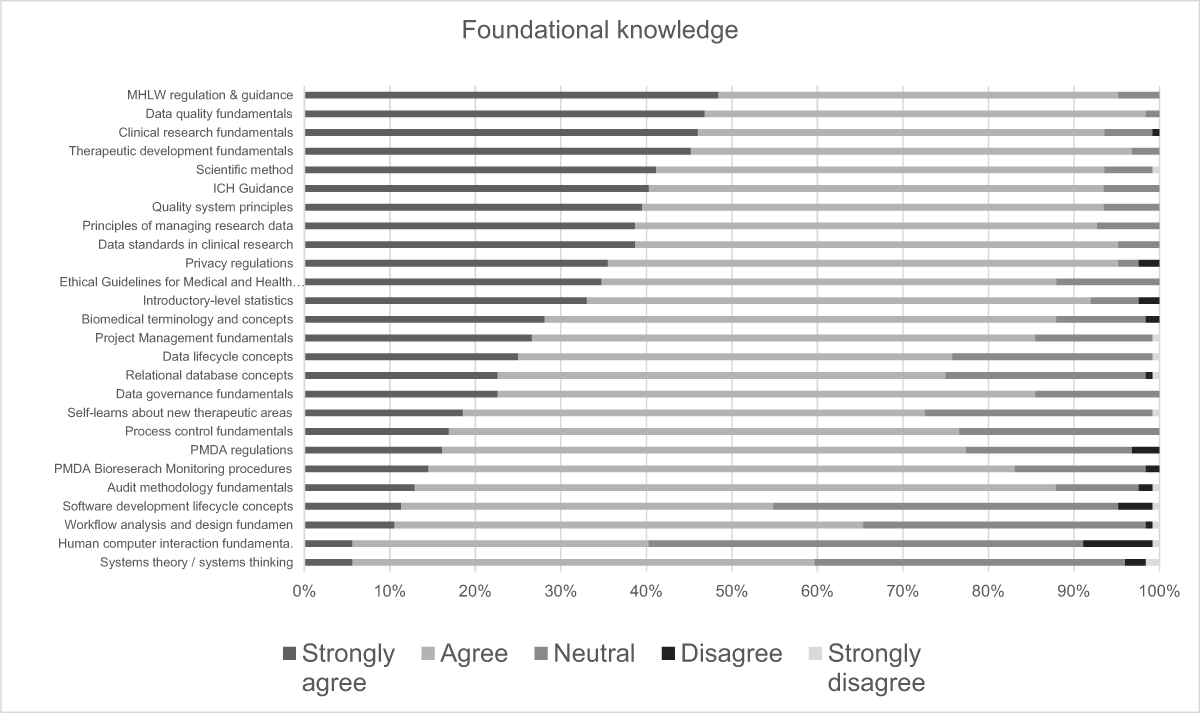
Foundational knowledge.
Discussion
In our survey of globally implemented competencies, we focused on the SCDM and the JTF Core Competencies. The reason for this is that although these two competencies are not yet well known in Japan, we believe that they are essential for investigating the development of a foundation for academic and pharmaceutical research and design from Japan to the rest of the world. For these two competencies, we consider the JTF competency to be an interprofessional collaborative competency and the SCDM competency to be a CDM specialized competency in clinical data management. We therefore believe that domain 1 “Scientific Concepts and Research Design” and domain 6 “Data Management and Informatics” of the JTF competency have a high affinity with the SCDM task competency.
In particular, while the SCDM task competency surveys have been implemented twice (at the 2015 and 2018 SCDM annual meetings), the number of CDM personnel from Japan that participate in such annual meetings is usually around 20–30; we therefore thought it necessary to prove if the SCDM task competencies can be directly applied to the task competencies of CDM personnel in Japan.
Although it was a short-term survey, we were able to evaluate the actual situation of CDM personnel with various backgrounds in the domestic industry and in academia (Table 2). The fact that this was achievable could be due in part to the well-functioning CDM network within the SCDM Japan Chapter, ARO and pharmaceutical companies, as well as the fact that CDM personnel in Japan are very interested in the competencies in their work. It is true that there was a slight bias in the responses, with most of the respondents from academia in the “early-to-mid” career groups and those from pharmaceutical companies in the“mid-to-late” career groups, however this may be directly related to the distribution of human resources. In academia, the distribution of respondents may be because human resource development is still in its infancy.
The differences in the SCDM CDM tasks between the two CDM carriers (Figure 1 and Supplemental Table 1) are very similar to the carrier-specific CDM tasks previously reported by Zozus et al.5 The JTF competencies (Table 3) also showed differences between the two carrier groups in similar subdomains, such as scientific design, quality control procedures, and leadership and professionalism. While multiple comparisons were conducted in the analysis, this study is essentially exploratory in nature. Even if the Bonferroni correction were applied to adjust for multiple testing, many items clearly demonstrated significant differences between the two groups. The alignment of the two competencies was also confirmed. This indicates that there are differences in the competencies of the CDM tasks that CDM personnel engage in daily, according to their career level. Differences in the tasks routinely engaged in by “mid-to-late career” and “early-to mid career” respondents included tasks in the design phase prior to the conduct of clinical trials, CDM project management tasks that are central to the work during implementation, review tasks at the end of the trial, and most data management tasks. These tasks are related to supervisory and management competencies, which are competencies that need to be acquired not only through knowledge but also through on-the-job training and experiences. Differences in CDM tasks among AROs, CROs, and Pharmaceuticals were also identified. In Pharmaceutical companies, where New Drug Application (NDA) products are often handled, project management is more rigorous and design tasks, such as determining data standards, are more common than in AROs (Supplemental Table 3). In addition, the analysis of the types of data managed (Supplemental Table 4) reveals a significant trend in data types handled by early-to-mid and mid-to-late career personnel. Our findings indicate that CDM personnel, regardless of their career stage, predominantly manage clinical data from CRFs, with a higher engagement observed in mid-to-late career personnel in managing complex data types such as ePRO, clinical lab data, data from central reading centers, and data from personal wearable devices.
It is suggested that the results of this study will have a significant impact on the future development of an evidence-based and competency-based CDM education curriculum in Japan. Yamaguchi et al.11 have been continuously conducting training workshops that target clinical data management professionals in academia. The results of this competency survey are currently being utilized in the educational programs for clinical data managers in academia in Japan as self-learning management tools to assess understanding.
The results on the types of data that were managed by CDM personnel (and the knowledge required to do so) were different in that they showed an increase in the use of new technologies, such as ePRO, eSource, RWD, and new clinical data management methods, when compared to the previous study. We think this is due to three reasons: eSource and artificial intelligence (AI)/machine learning (ML) are not utilized in that many clinical trials, there are not enough guidelines from regulatory authorities, and system vendors were not included in this survey. The reason why Japanese CDM personnel are not currently engaged in RWD work is thought to be that education of CDM personnel to date has been focused on regulatory and CDM procedures, and there are few opportunities for education in technology and computer science (Figures 2, 3). Ittenbach et al.12 propose a graduate-level curriculum in clinical data science that is specialized in the measurement, acquisition, management, treatment, and inference of clinical research data, as clinical data management evolves into clinical data science. In 2024, the SCDM also published a new Competency Framework,4 which highlights the increasing importance of AI/ML and data science skills for CDM personnel. The SCDM advocates that the competencies of future CDM personnel should include knowledge of ML and the use of AI for electronic medical record linkage and mass data processing methods, and also provides educational content.13
The survey also clarified several areas of basic education that are lacking in Japan’s CDM. Currently, there are only a limited number of university medical institutions in Japan that provide opportunities to learn about and gain skills in clinical data management as a professional learning course. One major challenge is that most educational materials, such as those provided by SCDM, are in English, which creates a language barrier that hinders widespread adoption among Japanese CDM personnel. Additionally, the current educational programs tend to focus on regulatory requirements and CDM procedures but lack content related to new technologies, such as eSource, AI, ML, and RWD. Furthermore, there is a shortage of mentors and trainers with expertise in these emerging fields, which makes it difficult to provide practical, hands-on training. Without addressing these challenges and creating comprehensive educational opportunities that include both foundational and advanced competencies, the future of CDM in Japan will remain limited.
Conclusion
This project clarified the competency-based tasks for CDMs in Japan. The key findings from this study are that significant differences exist in the tasks and competencies required at different career stages and types of organization. These differences must be considered when designing competency-based education and training programs to ensure that both early-career and mid-to-late career CDM personnel are adequately catered to the specific demands of their roles in Japan. This study provides the first formal documentation on this matter and serves as a crucial foundation for the development of future training programs that aim to enhance the overall competency of CDMs. By addressing the identified gaps in education and training, we can better prepare CDMs to meet the evolving challenges in clinical research, thereby contributing to the advancement of the field, both domestically and internationally.
Abbreviations
AI: artificial intelligence
AMED: Japan Agency for Medical Research and Development
ARO: academic research organization
CDM: clinical data management
CRF: case report form
CRO: contracted research organization
EHR: electronic health record
eSource: electronic source data
GCDMP©: The Good Clinical Data Management Practice
ICH-GCP: International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH) Guideline for Good Clinical Practice (GCP)
JTF: Joint Task Force
ML: machine learning
OJT: On the job training
SCDM: Society for Clinical Data Management
RWD: real world data
Additional File
The additional file for this article can be found as follows:
Supplemental File. Supplemental Tables 1 to 4. DOI: https://doi.org/10.47912/jscdm.355.s1
Acknowledgements
We thank Yukiko Matsushima, Mieko Inada, and Kanae Hirase for advising us on the importance of clinical research quality management competencies, from the perspective of clinical research associates (CRAs), and for collaborating on the translation of the JTF competencies during the CDM competency assessment. We thank Yasuko Matsuno for assistance with the administrative procedures of our project during the AMED ARO functional evaluation project. We thank Professor. Zozus for providing some insights into the CDM competencies regarding the current results from the perspective of previous reports. We also thank the SCDM Japan Committee for collaborating with this survey.
Funding Information
This analysis was supported by the grant from Japan Agency for Medical Research and Development.
Competing Interests
The authors have no competing interests to declare.
References
1. Joint Task Force for Clinical Trial Competency. https://mrctcenter.org/clinical-trial-competency/ Date accessed: 20 September 2024.
2. Sonstein SA, Jones CT. Joint task force for clinical trial competency and clinical research professional workforce development Front Pharmacol. 2018 Oct 16; 9: 1148.
3. Society for Clinical Data Management. https://scdm.org/ Date accessed: 20 September 2024.
4. CDM Competency Framework. https://scdm.org/cdm-competency-framework/. Date accessed: 20 September 2024.
5. Zozus MN, Lazarov A, Smith LR, Breen TE, Krikorian SL, Zbyszewski PS, Knoll SK, Jendrasek DA, Perrin DC, Zambas DN, Williams TB, Pieper CF. Analysis of professional competencies for the clinical research data management profession: implications for training and professional certification. J Am Med Inform Assoc. 2017 Jul 1; 24(4): 737–745.
6. eSource Implementation in Clinical Research: A Data Management Perspective, A White Paper June 12, 2014: SCDM. https://cdn.fs.pathlms.com/krzhNCoqRt6iFVLzZs7j?cache=true. Date accessed: 20 September 2024.
7. eSource in Clinical Research: A Data Management Perspective on the Use of Mobile Health Technology, A White Paper September 30, 2016: SCDM. https://cdn.fs.pathlms.com/84do5ymqQ0Gaqw3i3kOj?cache=true. Date accessed: 20 September 2024.
8. The Good Clinical Data Management Practice (GCDMP©). https://scdm.org/gcdmp/. Date accessed: 20 September 2024.
9. Valenta AL, Berner ES, Boren SA, Deckard GJ, Eldredge C, Fridsma DB, Gadd C, Gong Y, Johnson T, Jones J, Manos EL, Phillips KT, Roderer NK, Rosendale D, Turner AM, Tusch G, Williamson JJ, Johnson SB. AMIA Board White Paper: AMIA 2017 core competencies for applied health informatics education at the master’s degree level. J Am Med Inform Assoc. 2018 Dec 1; 25(12): 1657–1668.
10. Watanabe H, et al. Clinical Research Data Manager Training Curriculum Syllabus in Japan. Jpn J Clin Pharmacol Ther. 2020; 51(1): 19–46.
11. Yamaguchi T, Yaegashi H, Chiu SW, Uemura Y, Kawahara T, Miyaji T, Mashiko T, Takata M. The development and analysis of a Japanese modern comprehensive clinical data management training program. Heliyon. 2024 Mar 15; 10(6): e27846.
12. Ittenbach RF. From clinical data management to clinical data science: Time for a new educational model. Clin Transl Sci. 2023 Aug; 16(8): 1340–1351.
13. SCDM Learning Hub. https://learning-scdm.org/. Date accessed: 20 September 2024.